

BY PRIYANKA VERMA
Priyanka Verma is a second-year MA candidate concentrating in international development. Priyanka began her career as a graduate analyst for the Royal Bank of Scotland on the debt capital markets desk, where she helped advise on infrastructure and water utility deals. Most recently, she also worked with Shujog Impact Investments in Singapore and was involved with capacity-building work of social enterprises across Asia. Priyanka received her BSc in economics and statistics from the University College of London.
Over the last few decades Bangladesh has made huge strides in improving its sanitation coverage through an innovative community based approach. Much of this improvement has come from reducing open defecation and shifting the population to a shared latrine system. Going forward, however, the sanitation policies that enabled this success—relying on decentralized service delivery and extensive participation of non-governmental organizations (NGOs)—may prevent further mobility up the sanitation ladder.
Bangladesh’s Sanitation Policy
While the ultimate responsibility for sanitation services lies with the Ministry of Local Government, Rural Development and Cooperatives, the actual delivery of services has become increasingly decentralized over time. Local communities hold greater responsibility for operating and maintaining services by charging their own tariffs and establishing water committees to supervise sanitation related activities (Local Government Division 2011). Additionally, the government encourages NGOs and private sector involvement in sanitation development. The role of NGOs and the private sector is explicitly stated within the sanitation policy framework and improving the climate for private sector investment is one of its main objectives (Local Government Division 2005). Figure 1 illustrates the types of provider (public, private local, user association or NGO) involved in different parts of the sanitation value chain. The table demonstrates both the level of decentralization in Bangladesh and the prominent role private and NGO actors play in delivering sanitation.

Figure 1: Extent of provider Involvement in Sanitation. Source: WSP, 2007
The Shared Latrine Trap
Between 1990 to 2012, sanitation coverage in Bangladesh improved in both rural and urban areas (definitions of ‘improved’ and ‘unimproved’ sanitation are illustrated in figure 2). As shown in Figure 3, ‘improved sanitation’ coverage increased from 33% in 1990 to 57% in 2012 for the total population. The greatest success came in reducing open defecation from 34% in 1990 to just 3% in 2012. This is seen in both urban (figure 4) and rural (figure 5) sanitation, where open defecations levels have been brought down drastically.

Figure 2: The sanitation ladder. Source: WHO/UNICEF JMP
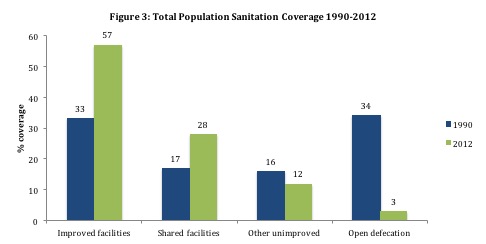
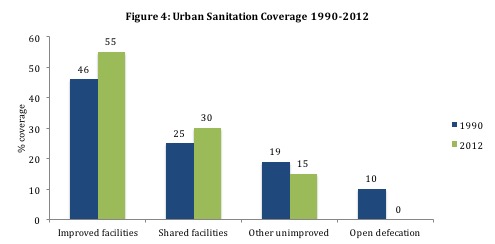
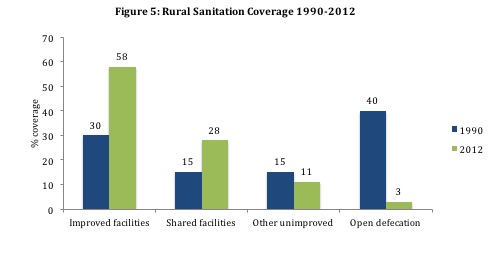
These figures seem promising at first glance, but the increase in rural and urban use of ‘shared latrines’ suggests that much more still needs to be done. It seems that a large portion of the improvement seen in Bangladesh’s declining open-defecation rates has been by shifting the population to a shared latrine system. Shared latrines – while better than open defecation – are not considered ‘improved’. This is because they are hard to keep clean, fill up faster because more people are using them and often need to be reconstructed once filled (Colin 2009). Most households using single pits will revert to open defecation once it is filled (Colin 2009). The pervasiveness of the shared latrine needs to be urgently addressed because this is not a sustainable method of sanitation delivery.
Additionally, Dhaka is the only urban area that has a conventional sewer system and even there it serves only a quarter of the population. It collects three times more waste than the capacity of the only existing wastewater treatment plant, resulting in untreated waste being discharged into the Buriganga river (Water & Sanitation Program 2014). Conditions in urban slums, where only 8-12% of households own hygienic latrines, are particularly inadequate and the increasing urbanization rates in Dhaka will further deteriorate sanitation conditions (Local Government Division 2005).
Decentralization – An Effective Policy Prescription?
Bangladesh’s success in reducing open defecation has been attributed to the Community Led Total Sanitation (CLTS) approach. CLTS focuses on community-wide behavioral change rather than just toilet construction. It seeks to raise awareness that even if a minority continues to defecate in the open, everyone is at risk of disease. Community-led methods, such as participatory mapping and analyzing pathways between feces and mouths (fecal-oral transmission of disease), are a means of triggering communities into action. CLTS has not only made users the direct stakeholders of their own sanitation but has created a sense of communal responsibility (Fawzi 2010).
One disadvantage of Bangladesh’s decentralized sanitation strategy, however, is the lack of accountability of NGOs. Unlike public organizations, which are directly accountable to the electorate, NGOs often have an obligation towards donor agencies, which can create misaligned incentives. These agent-principle issues are heightened by the growing oligopoly of the NGO sector. For example, only three organizations (BRAC, Proshika and ASA) account for 60% of all NGO membership and only eight receive 60% of total foreign funds – making many of these organizations too powerful to be held accountable by the poor (Local Government Division 2011).
Crowding Out Real Structural Reform
The large NGO and private sector participation disincentivizes the government from creating sustainable improvements in sanitation delivery. Hirschman’s framework of exit and voice illuminates this failure. When faced with deteriorating quality of public service, citizens have two options: they can either exit (withdraw from the service) or voice their grievances and proposals (Hirschman 1970).
The decentralized system has increased citizens’ use of exit but simultaneously decreased their voice. Bangladesh has over 3000 private sani-marts and more than 625 NGOs selling latrines (Water & Sanitation Program 2011). Thus, customers can easily exit by moving to another latrine seller. However, voice is decreased because they do not elect these NGOs and have no political leverage over them. By decoupling services from politics, the system may in the end also result in less politically active citizens (Haque 2002).
The increase in exit and the decrease in voice help explain the increasing use of shared latrines and the failure to move up the sanitation ladder to ‘improved sanitation.’ When ‘exiting’, customers simply move from one existing service to another, but they do not actually improve the overall quality of the options available to them. As Hirschman points out, when goods are provided by monopolies (as is the case for public services with only one government provider) voice can be a strong tool to actually increase quality (Hirschman 1970). In the case of Bangladesh, the government is not incentivized to make the structural changes needed to shift from shared to improved sanitation. NGOs and private sectors act as stop-gaps, providing the public with enough options so that they no longer feel the need to demand real structural change.
Moving Up The Sanitation Ladder, Sustainably
While Bangladesh has been a success story in reducing open-defecation, much remains to be done if these gains are to be economically and environmentally sustainable in the long term. The municipal sewage network needs to be expanded, which requires large infrastructure outlays and upgrades. Slum areas need to be addressed with a pro-poor slum policy that integrates water and sanitation solutions. Finally, a robust regulatory mechanism needs to be in place to ensure NGO and private sector accountability. These changes will require greater government participation on all levels. It remains to be seen if the state will be incentivised to step in and pull Bangladesh further up the sanitation ladder.
SOURCES
Local Government Division. Ministry of Local Government, Rural Development and Cooperatives. 2011. Sector Development Plan (FY 2011-25): Water Supply and Sanitation in Bangladesh.
Local Government Division. Ministry of Local Government, Rural Development and Cooperatives. 2005. National Sanitation Strategy. http://www.dphe.gov.bd/pdf/MR11_SanitationStrategy.pdf
Colin, Jeremy. 2009. “Sustainability and equity aspects of total sanitation programmes: A study of recent WaterAid - supported programmes in Bangladesh.” WaterAid
Water & Sanitation Program. 2014. “Benchmarking to Improve Urban Water Supply Delivery in Bangladesh”. Washington, DC: Water & Sanitation Program, World Bank.
Fawzi, Ammar and Hazel Jones. 2010. “Community-Led Total Sanitation (CLTS) for people in vulnerable situations Identifying and supporting the most disadvantaged people in CLTS - A case study of Bangladesh.” WaterAid.
Hirschman, Albert. 1970. Exit, Voice & Loyalties: Responses to Decline in Firms, Organizations and States. Cambridge: Harvard University Press
Water & Sanitation Program. 2011. “Scaling Up Rural Sanitation: Long Term Sustainability of Improved Sanitation in Rural Bangladesh.” Washington, DC: Water & Sanitation Program, World Bank.
Haque, Shamsul. 2002. “The Changing Balance of Power between Government and NGOs in Bangladesh.” International Political Science Review 23 (4): 411-435.